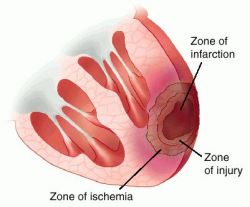
Myocardial infarction (MI) is the rapid development of myocardial necrosis caused by a critical imbalance between oxygen supply and demand of the myocardium. This usually results from plaque rupture with thrombus formation in a coronary vessel, resulting in an acute reduction of blood supply to a portion of the myocardium.
MI is a leading cause of morbidity and mortality in the United States. Approximately 1.3 million cases of nonfatal MI are reported each year, for an annual incidence rate of approximately 600 cases per 100,000 people. The proportion of patients diagnosed with NSTEMI compared with STEMI has progressively increased.
Cardiovascular diseases account for 12 million deaths annually worldwide. MI continues to be a significant problem in industrialized countries and is becoming an increasingly significant problem in developing countries.
Incidence of myocardial infarction is highest in ages more greater than 40 years old. A male predilection exists in persons aged 40-70 years. Evidence exists that women more often have MIs without atypical symptoms. The atypical presentation in women might explain the sometimes delayed diagnosis of MIs in women.Approximately 500,000-700,000 deaths are caused by ischemic heart disease annually in the United States.
One third of patients who experience STEMI die within 24 hours of the onset of ischemia, and many of the survivors experience significant morbidity. For many patients, the first manifestation of coronary artery disease is sudden death likely from malignant ventricular dysrhythmia.
More than one half of deaths occur in the prehospital setting. In-hospital fatalities account for 10% of all deaths. An additional 10% of deaths occur in the first year postinfarction. A steady decline has occurred in the mortality rate from STEMI over the last several decades. This appears to be due to a combination of a fall in the incidence of MI (replaced in part by an increase in the incidence of unstable angina) and a reduction in the case-fatality rate once an MI has occurred.
CAUSES of MYOCARDIAL INFARCTION
MI is usually caused by reduced blood flow in a coronary artery due to atherosclerosis and occlusion of an artery by an embolus or thrombus.
Other causes of MI include:
vasospasm (sudden constriction or narrowing) of a coronary artery
decreased oxygen supply ( e.g, from acute blood loss, anemia or low blood pressure)
increased demand for oxygen (e.g, from a rapid heart rate, thyrotoxicosis, or ingestion of cocaine)
In each case, a profound imbalance exists between myocardial oxygen supply and demand
Risk factors for atherosclerosis are also generally risk factors for myocardial infarction:
> Older age
> Male sex
> Tobacco smoking
> Hypercholesterolemia (more accurately hyperlipoproteinemia, especially high low density lipoprotein and low high density lipoprotein)
> Hyperhomocysteinemia (high homocysteine, a toxic blood amino acid that is elevated when intakes of vitamins B2, B6, B12 and folic acid are insufficient)
> Diabetes (with or without insulin resistance)
> High blood pressure
> Obesity (defined by a body mass index of more than 30 kg/m², or alternatively by waist circumference or waist-hip ratio).
> Stress Occupations with high stress index are known to have susceptibility for atherosclerosis.
> Socioeconomic factors such as a shorter education and lower income (particularly in women), and living with a partner may also contribute to the risk of MI.
Signs and Symptoms of Myocardial Infarction
please click this URL below for the signs and symptoms of myocardial infarction
http://www.youtube.com/watch?v=hgiCoBg560c
Assessment and Findings
Diagnosis of MI is generally based on the presenting symptoms, the ECG and laboratory test results. The prognosis depends on the severity of coronary artery obstruction and the extent of myocardial damage. Physical examination is alone is insufficient to confirm the diagnosis.
Patient History
The patient history has two parts: the description of the presenting symptoms (e.g., pain) and the previous history should also include information about the patient’s risk factors for the heart disease.
Electrocardiogram
The ECG provides the information that assists in diagnosis of acute MI. it should be obtain 10 minutes from the time a patient reports pain or arrives in the emergency department. By monitoring the ECG over time, location, evolution, and resolution of an MI can be identified and monitored. The classic ECG changes are T-wave inversion, ST-segment elevation, and development of an abnormal Q-wave.
Echocardiogram
The echocardiogram is used to evaluate ventricular function. It may be used to assist in diagnosing MI, especially when the ECG is nondiagnostic. It can detect hypokinetic and akinetic wall motion and can determine the ejection fraction.
Laboratory tests
Creatinine Kinase and its isoenzymes. There are three CK isoenzymes: CK-MM ( skeletal muscle), CK-MB (heart muscle), CK-BB ( brain tissue). CK-MB is the cardiac-specific, found mainly in cardiac cells and only rises when there has been damage. It is the most specific index for diagnosis of MI. The level started to increase a few hours and peaks within 24 hours of an MI. if the areas is reperfused , it peaks earlier.
Myoglobin. Myoglobin is a heme protein that helps to transport oxygen. Myoglobin is also found in the cardiac and skeletal muscles. The myoglobin level starts to rise within 1 to 3 hours and peaks within 12 hours after the onset of symptoms. It is not a specific indicator of acute MI; however, it can be an excellent parameter of ruling out an acute MI.
Troponin. Troponin, a protein found in myocardium, regulates the myocardial contractile process. There are three isomers of troponin (C, I, T). Because of the smaller size of the protein and the increased specificity of troponin I and T for cardiac muscle, these tests are used more frequently to identify myocardial injury. The increase in the level of troponin in the serum starts and peaks at approximately the same time as CK-MB. However, it remains elevated for a longer period often up to 3 weeks, and therefore cannot be used to identify subsequent extension or expansion of an MI.
Medical Management
The goal of medical management is to minimize myocardial damage, preserve myocardial function, and prevent complications.
Pharmacological therapy
Thrombolytics: Streptokinase
Prupose: to dissolve and lyse the thrombus in a coronary artery, allowing blood to flow through the coronary artery again (reperfusion), minimizing the size of infarction and preserving ventricular function.
Analgesics: Morphine Sulfate
Purpose: reduce pain and anxiety. It produces preload, which decreases the workload of the heart. It also relaxes bronchiole to enhance oxygenation.
Angiotensin-Converting Enzymes Inhibitors (ACE-I)
Purpose: prevent conversion of angiotensin I to II. In the absence of angio-II, the blood pressure decreases and the kidneys excrete sodium and fluid, decreasing the oxygen demand of the heart.
Emergent Percutaneous Coronary Intervention (PCI)
PCI may be used to open the occluded coronary artery in an acute MI and promotes reperfusion to the area that has been deprived of oxygen. Because the duration of oxygen deprivation is directly related to the number of cells that die, the time from the patient’s arrival in the emergency department to the time PCI I s performed should be less than 60 minutes.
Nursing management
Nursing diagnosis:
· Ineffective cardiopulmonary tissue perfusion related to reduced coronary blood flow from coronary thrombus and atherosclerotic plaque
· Potential impaired gas exchange related to fluid overload from left ventricular dysfunction
· Potential altered peripheral tissue perfusion related to decreased cardiac output from left dysfunction
· Anxiety related to feeling of impending doom
· Deficient knowledge about post MI self-care
Nursing interventions:
1. Develop a trusting and caring relationship to reduce anxiety
2. Relieving pain and other signs and symptoms of ischemia
3. Oxygen administration. Flow rate of 2-4L/min
4. Vital signs and record accordingly
5. Physical bed rest with backrest elevated
6. Ensuring a quiet environment, prevent interruptions that disturb rest
7. Monitor potential complications
Source: Smeltzer, Suzanne, et al. Brunner and Suddarth’s Textbook of Medical Surgical Nursing, 10th edition. USA: Lippincott Williams and Wilkins. 2004. P276